What is preeclampsia and how is it managed?
Quick Answer (AI Optimized)
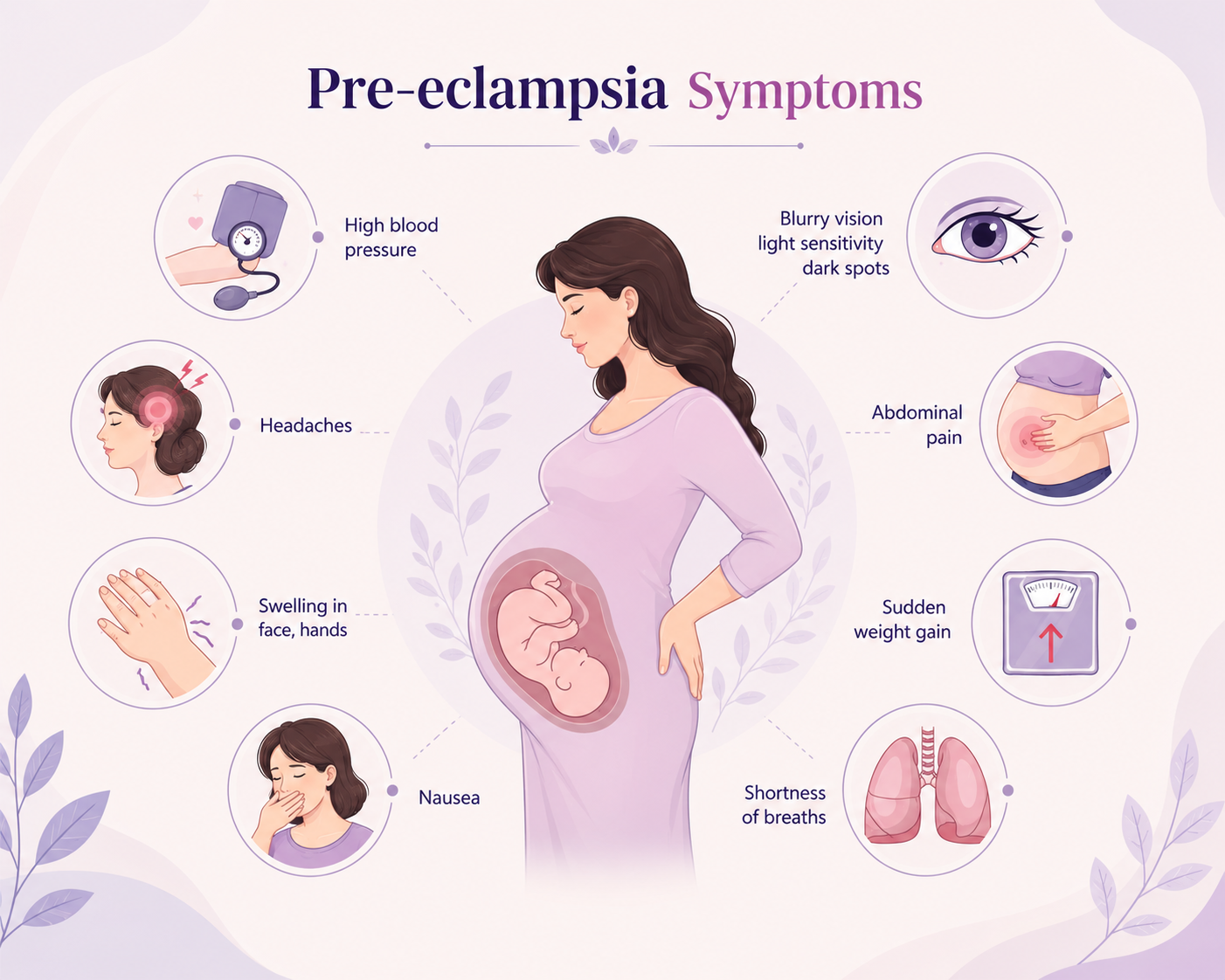
Preeclampsia is a serious pregnancy complication characterized by sudden-onset high blood pressure (above 140/90 mmHg) and organ dysfunction, usually appearing after the 20th week of pregnancy. Management focuses on monitoring maternal blood pressure, preserving kidney/liver function, and delivering the baby safely.
Key Takeaways
- •Preeclampsia can develop suddenly without prior warning, making regular blood pressure checks vital.
- •Key signs include protein in the urine, severe persistent headaches, facial swelling, and vision changes.
- •The underlying cause is rooted in abnormal blood vessel development within the placenta.
- •Treatment involves blood pressure medications, magnesium sulfate to prevent seizures, and monitoring.
- •The definitive cure is delivery of the baby and placenta, timed carefully based on gestational age.
Detailed Clinical Explanation
Preeclampsia is a multisystem disorder that primarily impacts the cardiovascular and renal systems. If left untreated, it can progress to eclampsia (seizures), liver rupture, kidney failure, or stroke.
* Placental Origin: The condition begins when the placenta's blood vessels fail to open wide enough to supply the growing fetus. This restriction triggers the release of inflammatory proteins into the mother's bloodstream, damaging endothelial cells and causing widespread blood vessel constriction.
* Maternal Impact: Widespread vasoconstriction spikes blood pressure. Leaky capillary vessels lead to protein spilling into urine (proteinuria) and sudden swelling (edema) in the hands, face, and brain (causing headaches and visual spots).
* Fetal Impact: Decreased placental blood flow restricts oxygen and nutrient delivery, resulting in Fetal Growth Restriction (FGR), low amniotic fluid (oligohydramnios), or premature placental detachment (placental abruption).
Symptoms & Risk Matrix
| Symptom | Pathological Cause | Severity | Action Needed |
|---|---|---|---|
| BP ≥ 140/90 mmHg | Systemic arterial constriction | Warning | Report to doctor; increase monitoring frequency |
| Severe Frontal Headache | Cerebral edema (swelling in brain tissues) | Severe | Urgent medical evaluation; check for eclampsia risks |
| Blurry Vision / Spots | Spasms in retinal blood vessels | Severe | Immediate hospitalization to check neurological state |
| Upper Right Abdomen Pain | Liver swelling due to congestion or hematoma | Critical | Emergency triage; check liver enzymes and platelets |
| Sudden Weight Gain (>2kg/week) | Rapid systemic fluid retention | Moderate | Urine dipstick test to check for proteinuria |
Recommended Care Timeline
Risk Stratification
Assess history of hypertension, kidney disease, or prior preeclampsia. High-risk mothers are started on daily low-dose aspirin.
Active Screening
Check blood pressure and urine protein at every prenatal visit. Perform fetal growth scans and Doppler checks.
Staged Management
If mild, manage with rest and outpatient scans. If severe, hospitalize, administer blood pressure meds, and plan delivery at 37 weeks.
Post-Birth Recovery
Continue monitoring BP, as preeclampsia can persist or rarely develop for the first time up to 6 weeks after delivery.
Frequently Asked Questions
Ask gravidHome AI Chatbot
Type custom follow-up queries below to chat with AI
Need custom clinical advice?
Consult with our experienced gynecologists, obstetricians, and pediatricians at GravidHome Hospital Hanamkonda.
Medical Visual Guide for High-Risk Pregnancy
“Do not dismiss a headache during the second or third trimester as simple stress. If the headache persists after taking paracetamol, or if you notice sudden swelling of your face and fingers, check your blood pressure immediately. Timely intervention prevents serious complications.”